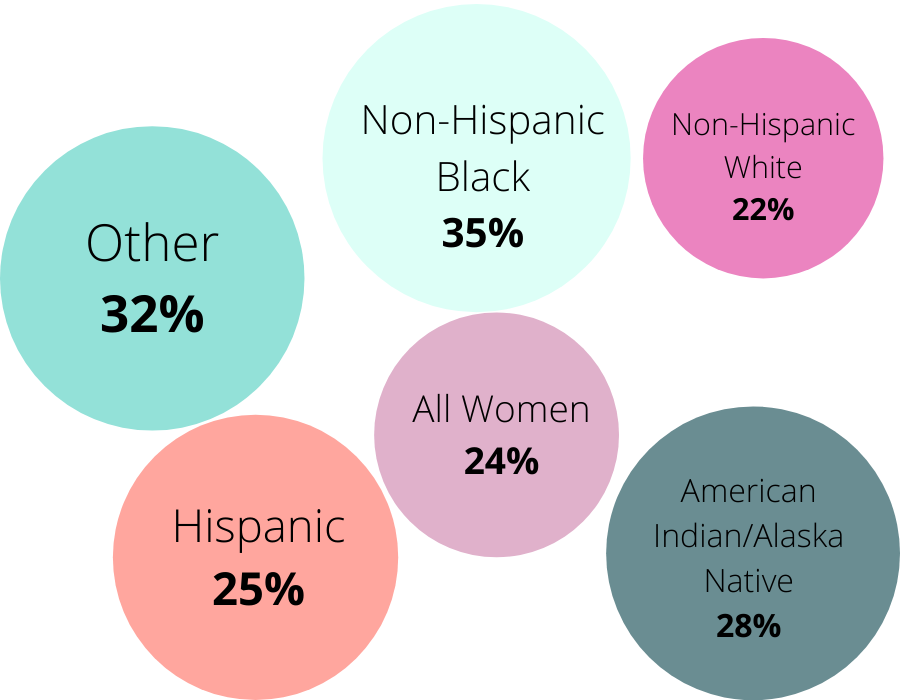
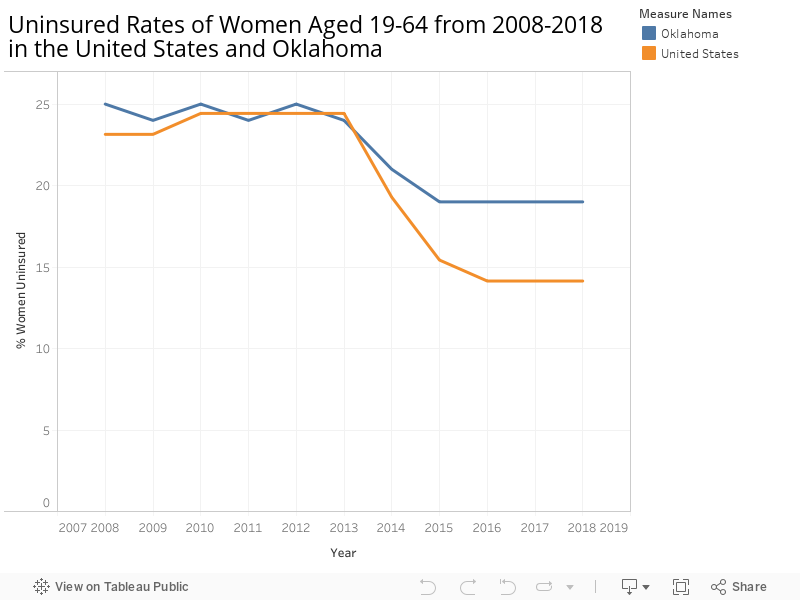
One of the most glaring barriers to care is the high number of uninsured women in Oklahoma. This percentage has stayed relatively stagnant over the last 6 years. Most people receive health insurance through their employer, but many people, including those who work part-time, or for small businesses, are often unable to get coverage.
On June 30th, 2020, Oklahomans voted to pass State Question 802 (SQ802). This amendment to the State’s constitution will expand Medicaid, also known as SoonerCare in Oklahoma, to provide healthcare to those who previously fell into the aptly named coverage gap. The coverage gap referred to the population with income between the current Medicaid eligibility level and the Federal Poverty Level, roughly between $5,104 and $12,760 for individuals. In Oklahoma, this means there are nearly 200,000 people who can now gain access to health care coverage!
Most are childless adults, who have been historically excluded from Medicaid eligibility. No one is more deserving of access to healthcare than another. Prioritizing access only when a woman becomes pregnant represents the pervasive belief that women’s health is restricted to motherhood. Policies like SQ802 will help all Oklahomans lead healthier, happier lives.
Questions still remain as to how exactly Medicaid expansion will happen. One proposed idea is to utilize a privatized managed care model, meaning healthcare services would be organized and delivered only through certain providers. However, this idea is hotly contested due to the potential harm managed care could cause to the interests of patients and providers alike. These conversations about accessing healthcare clearly aren’t over just because SQ802 passed.